
Introduction
Hydroxichloroquine (HCQ) is a common corticosteroid medication that is one of the primary drugs given to patients with autoimmune diseases to suppress the immune system and keep the body from attacking itself. It is somewhat less potent than other corticosteroids, but it is great for long-term usage. For quite a while, various researchers and doctors have noticed that patients with autoimmune diseases, such as SLE or RA, who take HCQ have a reduced risk of cardiovascular illness and complications. Though not all of the mechanisms are known, new evidence has shown that the reduction of cardiovascular risk originates, at least partially, from the effects of the drug that reduce the level of lipids and sugar in the blood. Furthermore, the study aims to test the theory of whether changes in blood pressure, heart rate, arterial stiffness, and strength could be responsible.
Methodology
The study sampled 45 people from Sweden, and ended up choosing 23 people with SLE and 7 people with RA. The people chosen for the study showed moderate disease activity, did not take significant amounts of prednisolone, and had not taken HCQ for at least 250 days before their inclusion in the study. Half of the people chosen were randomly selected to begin a 4-week-long HCQ treatment after a 4-week observation period, while the other half took 8 weeks of HCQ treatment.
At the start of HCQ treatment, four weeks after the start of treatment, and eight weeks after the start of treatment, blood pressure and heart rate were measured. Following overnight fasting, blood samples were analysed for measurement of total cholesterol, high-density lipoproteins (HDL), low-density lipoproteins (LDL), triglycerides (TG), apolipoprotein A1 (ApoA1), apolipoprotein B (ApoB), lipoprotein, blood glucose, glycated haemoglobin (HbA1c), and CRP. Blood pressure was measured in the form of pulse wave velocity (PWV). Arterial strength and stiffness were also measured separately.
Results
Various indicators of cardiovascular health can be seen in the following figure:
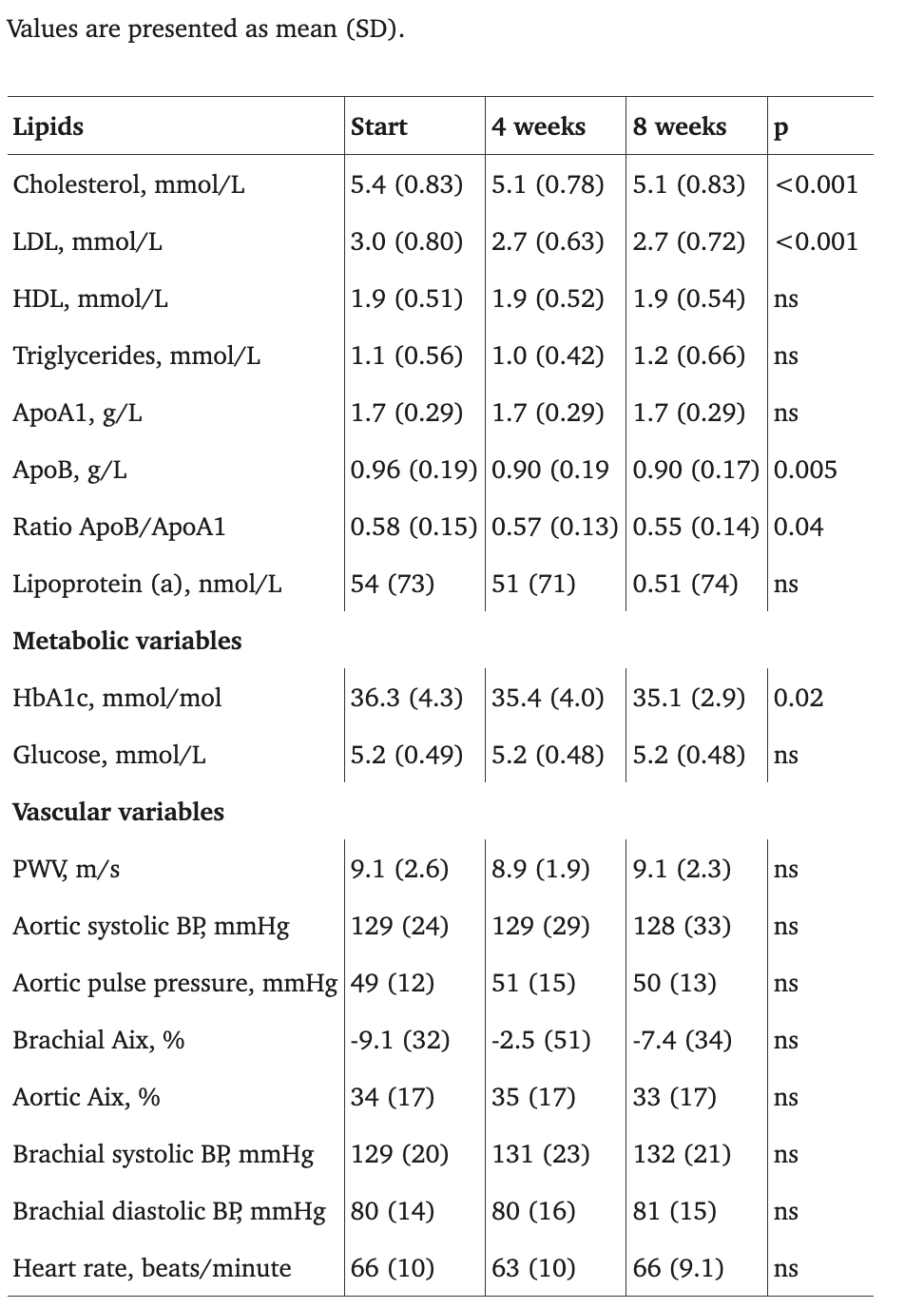
Table 2. Levels of lipid variables, metabolic variables, and vascular variables at the start of treatment with HCQ, after four weeks of treatment, and after eight weeks of treatment.
The data shows a very discernible drop in three variables: LDL, total cholesterol, and HbA1c. Very much in line with the drop in LDL, there is a very similar drop in ApoB.
There were no significant changes in PWV, aortic or brachial Aix, aortic blood pressure, or pulse pressure at any point of measurement. There was also no significant change in systolic blood pressure, diastolic blood pressure, or heart rate.
Conclusion
HCQ's effects on lowering blood sugar, LDL, and cholesterol are clear, but these factors alone do not fully explain the mechanism behind the high reduction in cardiovascular disease rate in autoimmune patients who take it. Factors like arterial strength were considered, but ultimately showed no changes under HCQ treatment. Although the study partially explains the HCQ's unique abilities, more study is ultimately needed, potentially into areas such as IL-1 signalling. Though the study has ensured that the odds of a null hypothesis for the effects on cardiovascular health in the study being true are statistically negligible (<5%), it is still somewhat limited by a smaller sample of patients that does not necessarily represent the entire population. Furthermore, some of the findings are not fully established through past research. Only one study before investigated the effects of HCQ treatment on blood pressure in people with rheumatic diseases. Last of all, the study recognizes its own potential cofounding factors, such as the fact that things like body weight and obesity were not taken into account, despite their noticeable effect on cardiovascular health.

