
Introduction:
Internal carotid artery stenosis occurs due to plaques at the part where the carotid artery splits, with risks increased with high blood pressure, age, male sex, diabetes, smoking, and chronic inflammation. Since microorganisms have been shown to possibly be inflammatory triggers, theories that these microorganisms can relocate from the mouth to the cardiovascular system and contribute to plaque formation have formed. This is further supported by the presence of oral pathogens such as Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans in arterial plaques. Previous cases have attempted to see if there was a relationship, but the sample size was extremely small or it was not compared to the subgingival environment.
Methods:
Between February 2019 and June 2023, 25 patients diagnosed with carotid artery stenosis and with at least four natural teeth or implants were chosen. Characteristics of each person were recorded, including their age, sex, smoking status, BMI, and medical history. Due to limitations such as X-rays not being able to be taken, Periodontal health was classified as severe, moderate, or mild/absent, based on clinical attachment loss, pocket depth, and tooth loss.
A sterile curette was used to take plaque samples after the biofilm was removed from all test teeth. Microbial DNA was extracted, and genetic sequencing of the V3/V4 region of the 16S rRNA gene was performed, creating taxonomic classifications based on a reference database known as SILVA. Alpha diversity and Beta diversity were calculated for each sample, along with the abundance of major taxa.
Results
The top ten most abundant phyla were recorded for subgingival samples and carotid stenosis samples, which can be seen below in Figure 1.
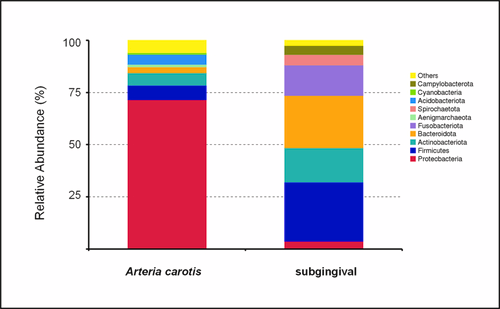
(Figure 1)
The subgingival samples contained 94 genera of bacteria, while the carotid samples had 84 genera. Seven genera were shared between the two samples.
Alpha diversity was lower in the carotid sample, which shows a lower diversity and less even spread of microbial genera, suggesting a more selective colonisation in the atherosclerosis plaques, as seen in Figure 2.
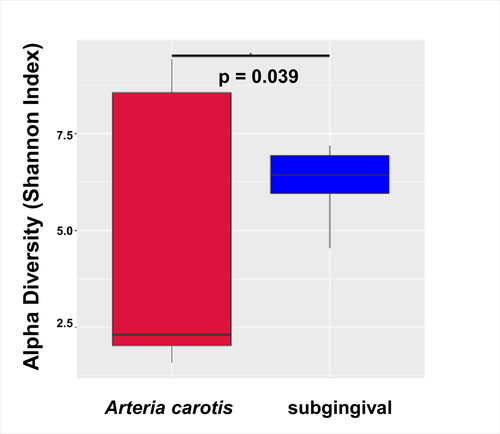
(Figure 2)
Beta diversity was higher in carotid samples, showing how Bacteroidota were dominant in oral samples while Proteobacteria were dominant in carotid plaque. Oral samples also had high variability between individuals, and Carotid microbes and microbiomes were different from oral samples and microbiomes.
While some individual species, such as Fusobacterium nucleatum, were detected in both samples, this only occurred in very small groups of people(less than 3) and so were considered isolated events that had no correlation.
A limitation to note is that while this study did include 25 patients, much more than any other case study on this subject, it is still limited and may not accurately portray a general population, giving it less statistical significance. There might be a lot of weight put on small overlaps of bacterial taxa in both samples due to the small sample size. There may also be contamination due to low biomass in atherosclerotic plaques.
Conclusion
The study essentially showed that while oral bacteria may travel through the bloodstream, atherosclerotic plaques harbored bacteria and microbes that are designed to survive under the oxidative and inflammatory conditions of the bloodstream. The low alpha diversity reinforces previous ideas of how plaques in the bloodstream have a less complex microbial community compared to the oral or gut microbiome, which is likely due to the harsher conditions of vascular tissue. The beta diversity proved that the two samples were different microbial ecosystems and mostly unrelated to each other.

