Introduction
Pediatric emergency department (ED) visits continue to increase, despite the rarity of severe infections. Early recognition of severe illness in children is challenging, even for professionals. With digital innovation, detection is now being improved; however, there is limited data on the parental aptitude for identification. Great parental concern has been associated with more severe illnesses. Mutual improvement is the best course of action. Professionals should take a parental word into account, and parents should do what they can to both trust the professional whilst providing helpful information.
Methods
The diagnostic accuracy of parents was evaluated in this study, using methods to identify which parental observations best predicted severe illness in children and adolescents with acute illness presenting to an ED. Taking place in Oulu, Finland, this study was approved by a Hospital Ethics Committee.
The study comprised 2375 pairs of either a child or an adolescent and their parent who visited the ED at a university hospital. The ED provided primary, secondary, and tertiary care for those with acute illness. Almost 8500 patients visited the ED during the data collection period. Other than an inability to communicate due to language gaps, no criteria were used to exclude any patients. 6048 of the pairs were not screened due to limited staff or urgency of the condition or crowding.
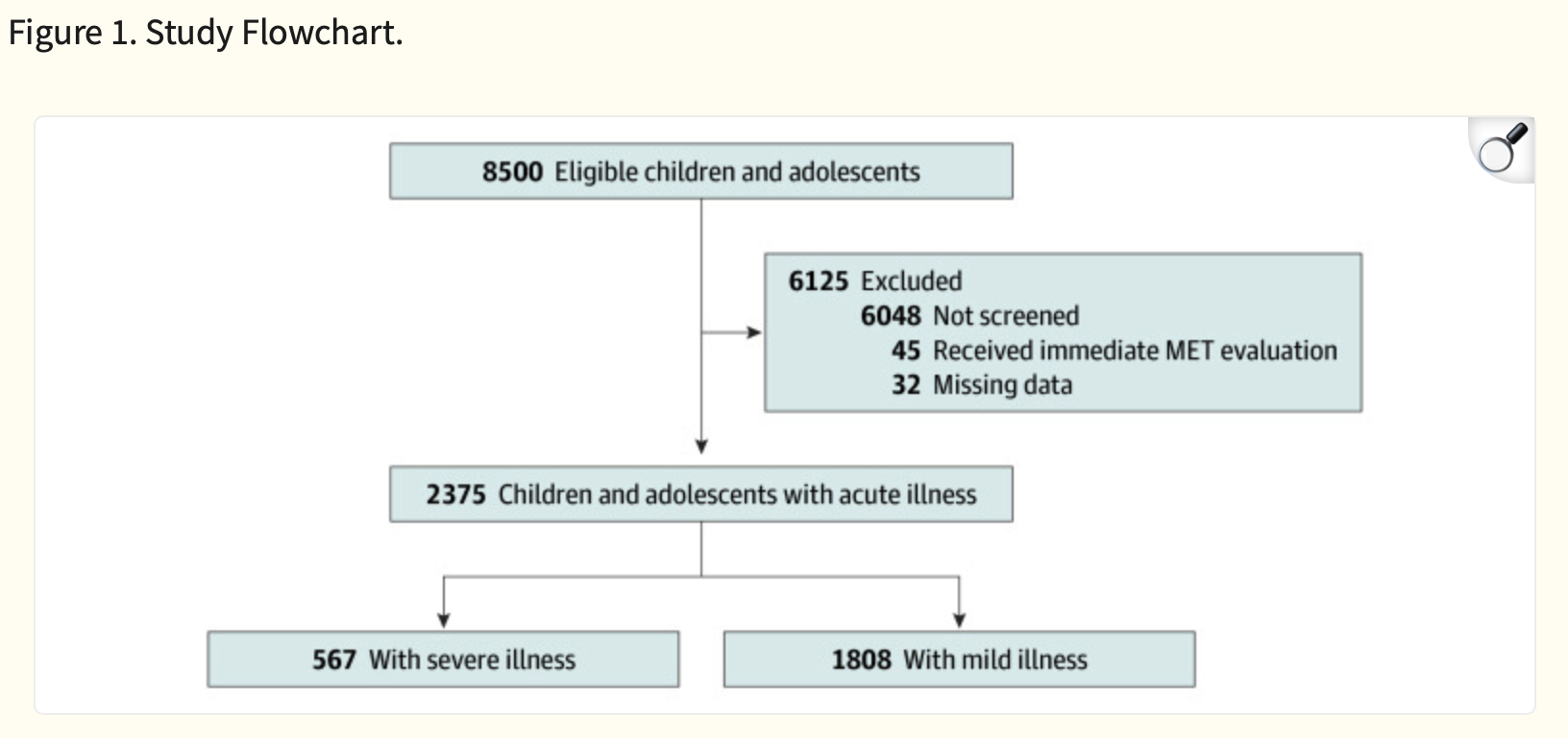
Shown above in Figure 1 is the breakdown of the subjects of the study, noting that MET stands for a medical emergency team. The final analytic sample consisting of 2375 children and adolescents with 567 (23.9%) having severe illness and 1808 (76.1%) having a mild illness.
Parents who agreed to participate were advised to complete the questionnaire alone or with their partner. 36 items were included, based on the child or adolescent's symptoms and the parent's observations. It included items derived from tools used by healthcare professionals to assess children or adolescents. Clinically relevant symptoms or previous illness severity scales were also inquired about. One questionnaire was provided per visit, and no further instruction was provided.
Severe illness itself was defined as 1 or more of the following: admission to pediatric intensive care unit (PICU), hospital treatment lasting more than 24 hours, need for intravenous or nasogastric fluids, required intravenous antibiotics for more than 24 hours, oxygen saturation less than 93$%, need for inhaled medications, anaphylactic shock, intoxication requiring admission, or surgery. Medical records ad histories were also reviewed.
An estimated minimum sample size was 257, with the most effective parents questions being associated with an increase in sensitivity and 2310 for specificity of severe illnesses. Specificity and sensitivity were then calculated with accuracy of parental observation.
Machine learning was utilized on the data to predict outcomes. characteristics of patients and irrelevant data was omitted. A simple score of 3 parental questions with the highest feature importance as decided by the machine learning was then calculated and evaluated.
Results
Within the studied group, the mean age was 5.4, with 48% of the subjects female and 52%. male. 35.4% o the patients were under 2 years old and 20.8% had an underlying illness such as allergies or asthma. 32.4% of the patients say symptoms within 24 hours of the arrival at the ED. 44.5% of patients were walk-ins without a referral, whilst 27.1% were referred by a primary care physician, 26% arrived after calling the phone service, and 2.4% were brought by emergency ambulance. Overall, 22.6% were admitted to the hospital and only 1.2% to the PICU. The common diagnoses included an upper respiratory tract infection (11.4%), abdominal pain (6.2%), fever (6.1%), and a lower respiratory tract infection/wheezing (5.3%).
Altogether, 23.9% met at least 1 criterion for severe illness, which were the same as those shown above (see Methods). 95.4% of parents responded to the final question, as many strived to complete the questionnaire. The degree of parental worry was the highest response rate, with most giving opinions on the necessity of treatment and whether their child was well enough to socialize or play. Lower response rates were seen in questions about whether the child was seriously ill, as well as specifics like tiredness whilst eating or crying patterns.
The machine learning showed specificity and sensitivity to have different levels of effectiveness for both individual pediatric and gut feeling questions, with the ranges of sensitivity and specificity differing heavily based on topic. Hospital admission was predicted with moderate accuracy, with the most important question for prediction being the parental opinion on the need for treatment. ICU admission was to a similar degree of accuracy with general appearance being the mot important question there. It is key to note that the machine did perform exceedingly poorly at predicting the hospital admission of children under 2 with fever related illness.
It is important to note the limitations of this study. It only took place in one area, northern Finland in one hospital. Any area-specific public health or internal issues could have impacted results. The impact of parents having to self-report also provides another factor which could cause error in the results. Furthermore, as seen, we do not have a complete data set, with multiple groups being rushed away before data was collected, or having missing information. No data on the parents and their own situations themselves were also collected.
Conclusion
In sum, whilst parental worry or gut feelings have excellent sensitivity, the specificity is very low. Poor diagnostic performances suggest false positives and prove that they cannot be used as a stand-alone decision tool in ED settings. Illness severity scoring systems have been developed to predict illnesses in children. A score system for parental use has also been in development. The study shows a valuable parental ability in identification of severe symptoms, and a standardized set of questions could jeopardize this. Simple questions are likely better. The digitalization using modeling was also shown to be helpful. However as noted before, young children were challenging to diagnose. Parental concern is a red flag, that is sure. However it should be interpreted alongside clinical assessment to avoid any unnecessary care. Digital tools in any form should be carefully validated before usage as well.
